.png)
When New York educators were asked at this year's Capital Region BOCES Social Emotional Learning Conference how many of them were dealing with attendance challenges in their districts, nearly every hand in the room went up. It was the kind of moment that feels less like a poll and more like a mirror.
The session that followed — When Mental Health Becomes the Attendance Strategy: District Leaders on Implementation & Impact — wasn't a presentation about what chronic absenteeism looks like. Most people in that room already know. It was a conversation about what it actually takes to do something about it, led by four district leaders who have been building that answer from the inside.
Jillian Kelton, M.Ed., Director of District Engagement at Cartwheel, moderated the discussion alongside:
- Kerri Canzone-Ball, Ed.D., Director of Pupil Personnel Services, City School District of Albany
- Marcie Bouchard, Districtwide Behavior Specialist, City School District of Albany
- Becky Dostie, School Counselor, Ryder Elementary School, Cobleskill-Richmondville Central School District
- Jeremiah Haslun, Middle School Principal, Cobleskill-Richmondville Central School District
"Here are some of the ideas that surfaced in that conversation.
Chronic absenteeism is a symptom. Treat it like one.
Across New York State, nearly one in three students is chronically absent — missing 10% or more of the school year. Behind that number is a large share of students for whom something — anxiety, family stress, a sense of disconnection, an unmet need that nobody has named yet — is making school feel impossible.
"Chronic absenteeism is almost never just about not wanting to come to school," Jillian told the room. "There is almost always an underlying reason why a student cannot — or does not feel comfortable — coming to school. And it's a signal."
For the districts in this conversation, progress began when they started treating attendance as a symptom of unmet mental health needs rather than a problem to solve directly. That reframe can change who owns the solution, which interventions get prioritized, and what progress looks like.
The post-COVID landscape made this reframing urgent. Becky Dotsie, working with elementary students in rural Schoharie County, described watching the pandemic fracture a developmental timeline her students are still catching up to. "It feels like COVID fractured a timeline," she said. "We reference things as pre-COVID or since. The impact we still feel — it's a lot."
Jeremiah Haslun, leading a middle school through those same years, watched it arrive as a surge of behavior referrals, disengaged students, and teachers asking for help they couldn't quite name. "Behaviors just skyrocketed," he said. "Teachers were scratching their heads saying, we don't know what to do here."
The problem isn't a lack of caring — it's a lack of infrastructure.
When the session polled the room on the single biggest barrier to mental health access for students, the results were telling:
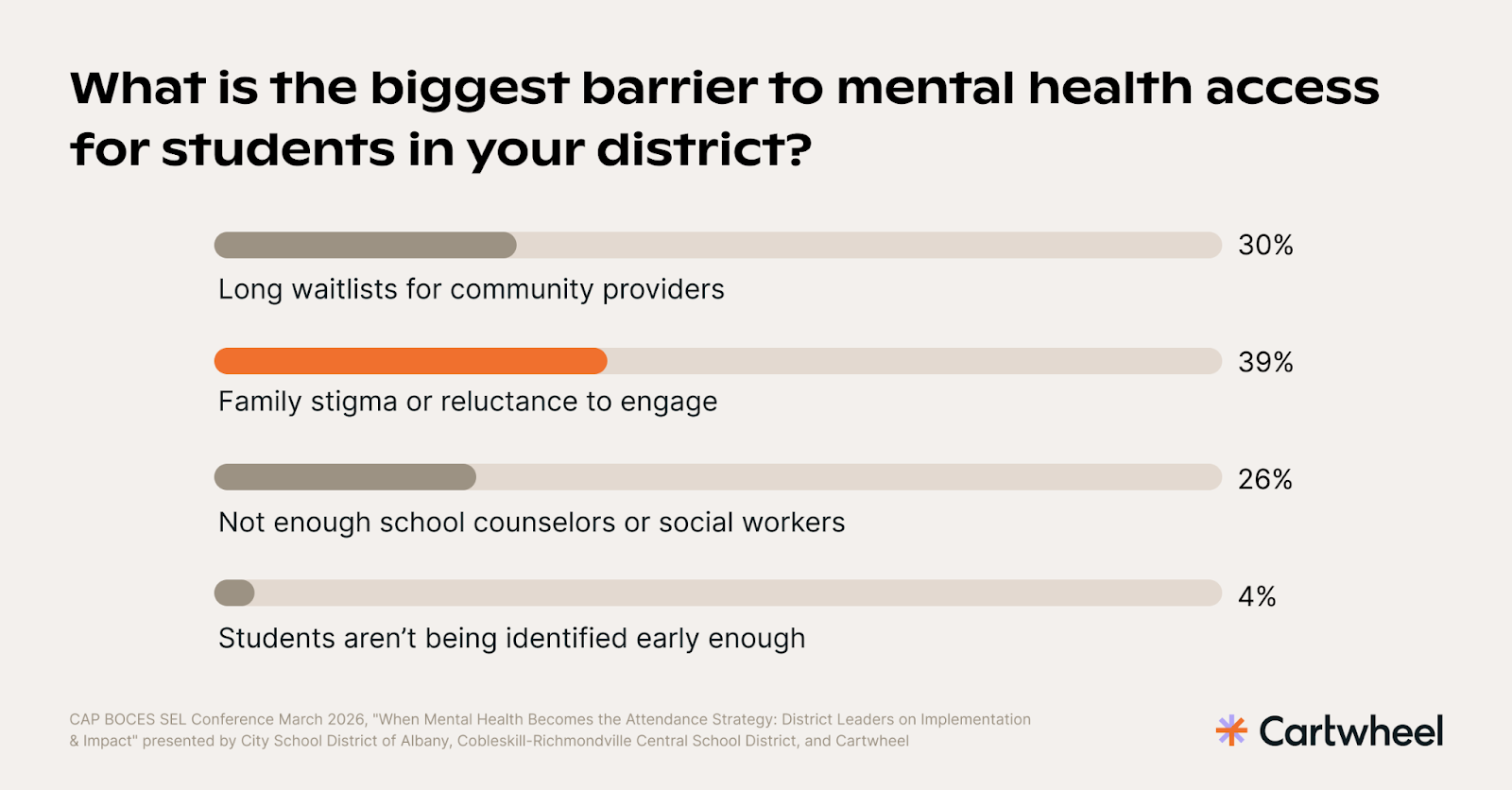
Nearly two-thirds of respondents pointed to family stigma or waitlists — barriers that effort and caring alone cannot fix. They often require structural solutions.
Jillian Kelton drew the parallel directly: "If a student needs reading support, that student gets access to a reading specialist. Their progress is tracked. If it's not working, they shift the intervention. Can we say the same happens for mental health supports in our schools?" The answer, she noted, is almost universally no — not because of a lack of will, but because schools were never built with that infrastructure in place.
What Albany and Cobleskill-Richmondville share is a decision to stop waiting for that infrastructure to appear and start building it with what they had. Albany already had a robust continuum — co-located behavioral health clinics in secondary buildings through a 30-year partnership with Northern Rivers Family of Services, a full student support team in every building, and a $2.5 million OMH grant supporting a psychiatric nurse practitioner and mobile crisis response. But even with all of that, Marcie Bouchard described a district with more need than coverage. Elementary buildings had limited clinic access. Community providers were closing. Staff were identifying students who needed help and hitting dead ends. "We used to have a list of all these mental health providers we could call," Marcie said. "We couldn't keep up with it — frequently you'd call and the place wouldn't even exist anymore."
Cobleskill-Richmondville's landscape was starker. Mental health waitlists in Schoharie County can run six months to a year. For families spread across a large rural area, getting to an appointment meant a long commute often to a facility that serves a range of court-ordered and clinical populations, not just counseling. In a small community where everyone knows everyone, there's a stigma around being seen in a clinical office — families don't want to be seen walking into a therapist's office. And for some families, access to a device or reliable internet wasn't a given. Every one of those barriers — the wait, the distance, the stigma, the technology gap — had to be part of the solution.
Both districts expanded capacity by adding Cartwheel as a telehealth partner — not as a replacement for what existed, but as a way to reach students and families the current system wasn't reaching. As Jillian framed it: "This is a solution. It is not the solution." The value is in expanding the toolbox, not in any single tool.
Family trust isn't just a communications strategy — it's a clinical one.
When the room was polled on their biggest challenge with family engagement around mental health, the leading answer wasn't stigma or awareness. It was logistics.
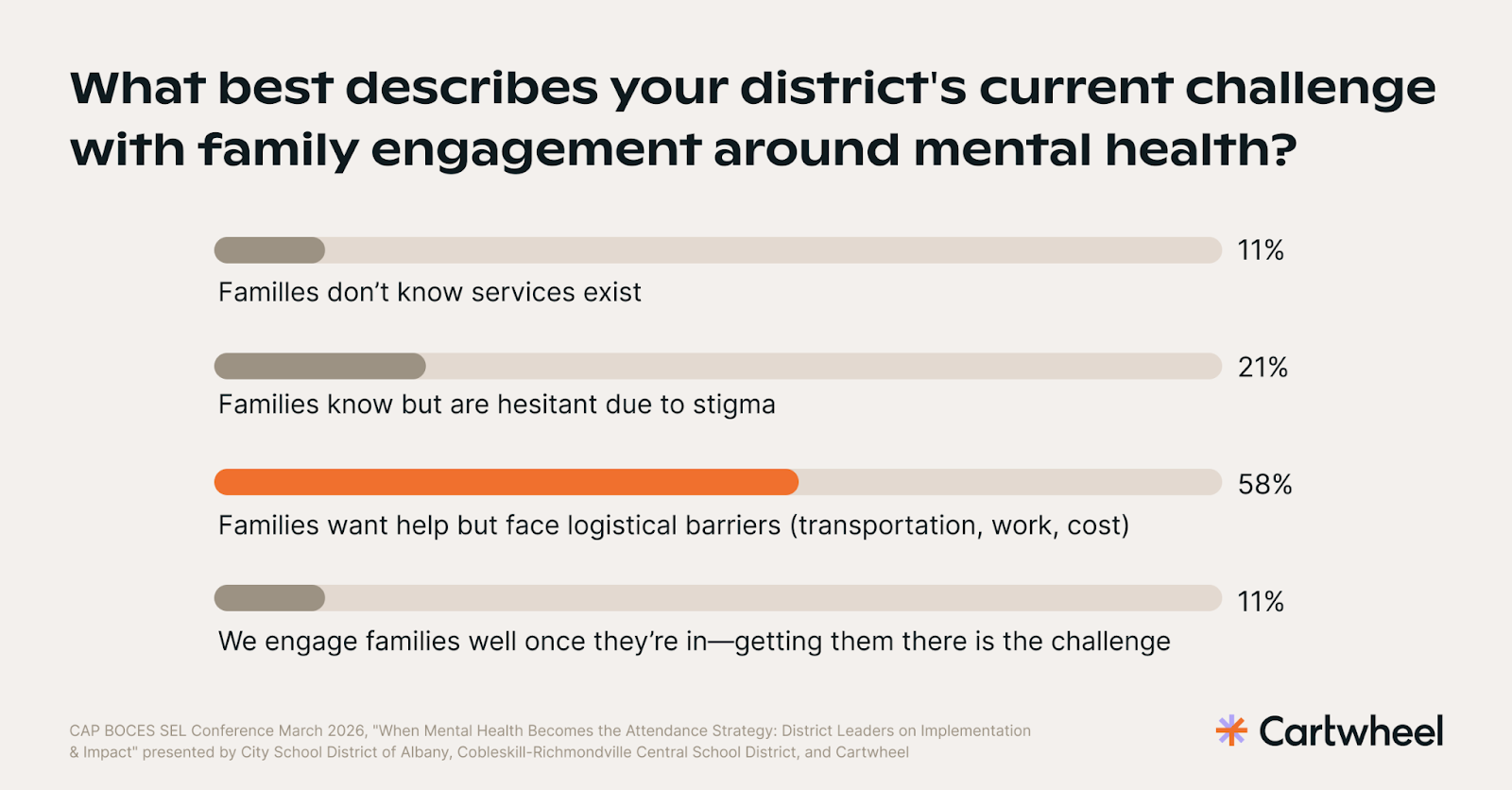
Fifty-eight percent said families want help but can't get to it. That suggests the barrier is less about reluctance and more about access. Albany serves families navigating immigration concerns, housing instability, and significant community trauma, with over 150 languages spoken across its student population. Building trust with those families required sustained, visible commitment: community roundtables, a Parent University series, and persistent communication to keep services visible at the school level. "We can't stand behind advertising Cartwheel if we didn't believe in it," Kerri said. "We've helped hundreds of kids access their education and become successful by providing services like these."
One of the more significant moves was a family interest form — a direct way for families to request services on their own terms, without going through the school first. Roughly 25% of Albany's referrals now come through that form, a sign that families are actively seeking support, not just waiting to be referred.
In Cobleskill-Richmondville, Becky described the same principle at a smaller scale: monthly wellness-themed communications sent to all families, each one noting that families can reach out directly for services. The results surprised her. "In some cases, the families who signed up were ones we didn't even know were struggling," she said. "That's why I say cast a broader net — we don't know what we don't know."
When families are partners in their child's care — not just people signing a consent form — students are more likely to improve — and more likely to show up. In Cobleskill-Richmondville, 88% of parents with a child in Cartwheel services reported being very or extremely satisfied with the experience of getting started. In Albany, 80% of students are showing meaningful improvement in mental health symptoms. Those numbers reflect what happens when a family trusts the process enough to stay in it.
Sustainable funding is a question every district is asking.
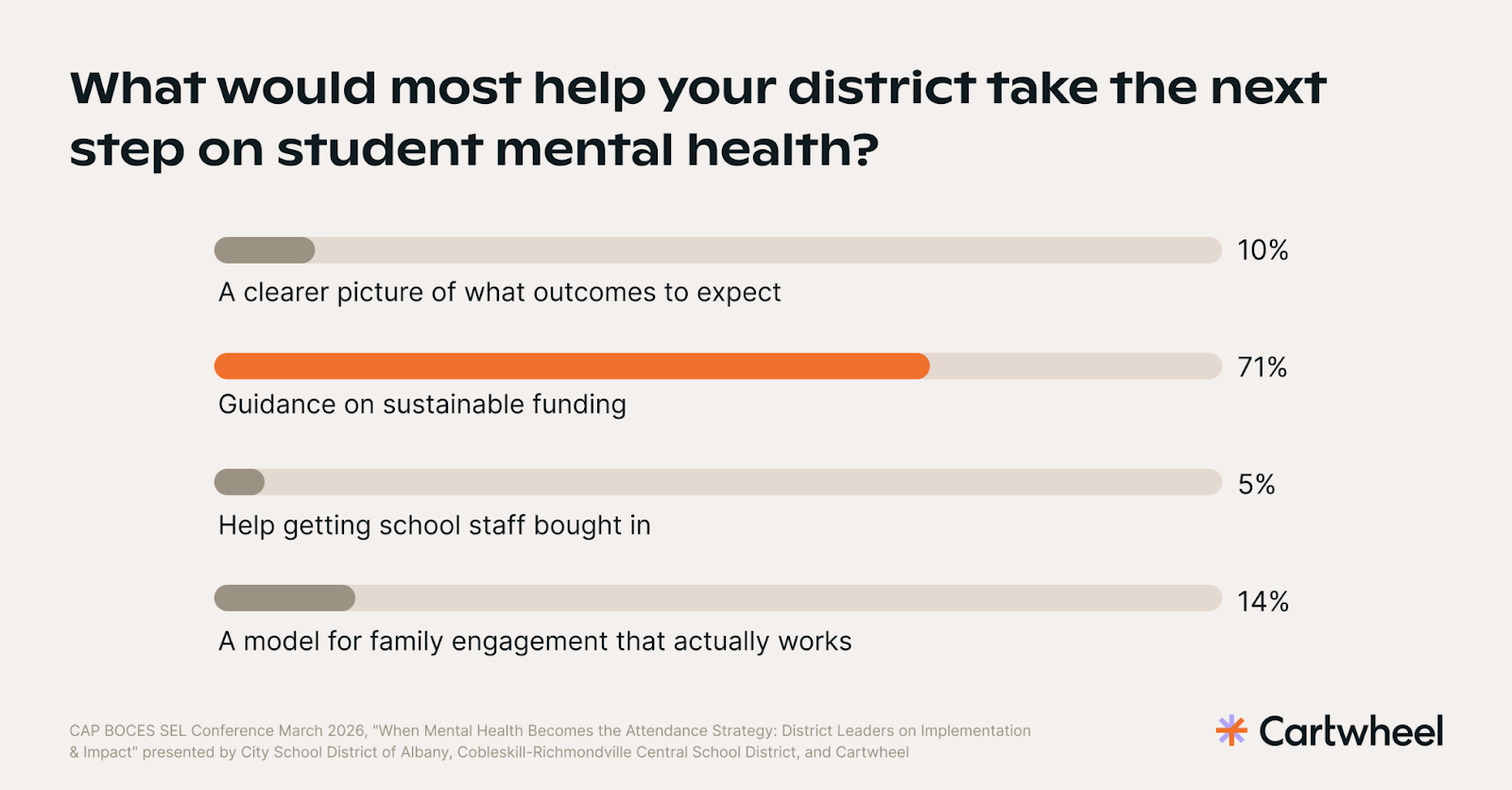
71% of educators in the room said guidance on sustainable funding was the most important next step their district could take on student mental health — more than staff buy-in, family engagement models, and outcome clarity combined.
Kerri Canzone-Ball, navigating a district budget facing a potential $10–12 million shortfall, was candid: mental health infrastructure has to be argued for in the language of outcomes that boards actually track. "You can have every academic resource in the world and the best people in front of your kids," she said. "But if students aren't feeling emotionally safe and connected, they are not going to produce academic achievement." That's the argument — and the data supports it.
Cartwheel's research with Peoria Public Schools found a 44% reduction in chronic absenteeism among students receiving services, which represents an average of 10 additional instructional days per student, alongside a 68% reduction in suspension rates. A comparable group that didn't receive services saw no similar improvement.
The funding model matters here too. Because Cartwheel bills insurance directly, districts aren't dependent on grant cycles to sustain the partnership. For families with Medicaid, services are often at no cost to the family or the district. In New York, districts contracting through BOCES can access state aid on their Cartwheel agreements — making this a partnership that fits within existing procurement structures rather than requiring new budget line items.
Albany is already building the case for Cartwheel as an attendance intervention — aligning it with attendance-focused funding streams and presenting outcome data to leadership and the board. "Those data points are irrefutable," Kerri said. "Start where you can. Don't wait for the perfect funding picture."
What makes this work: three things to take back
Building a sustainable school mental health program in New York requires more than finding the right clinical partner — it requires the right internal infrastructure. Districts that are seeing early progress share a few things in common:
- Make it easy for families to find you — not just for staff to refer. Albany's family interest form now accounts for roughly 25% of referrals — families actively seeking support on their own terms. In Cobleskill-Richmondville, monthly wellness communications led families to sign up who the district didn't even know needed help. When families have a direct path in, you reach students the referral system misses.
- Name a coordinator and build it into your MTSS structure. Someone needs to own the referral flow, troubleshoot with families, and keep the program visible across buildings. In Jeremiah's building, teachers now raise Cartwheel at MTSS meetings the same way they'd raise a reading intervention — that shift from last resort to natural option doesn't happen on its own.
- Start building the funding case now. Seventy-one percent of the room said sustainable funding was their top need. Because Cartwheel bills insurance directly, districts aren't dependent on grant cycles — and in New York, BOCES contracts can access state aid. Kerri's advice: "Start where you can. Don't wait for the perfect funding picture."
When mental health becomes part of your attendance strategy, it can change what's possible for students and families. See how Cartwheel supports New York school districts.





.png)
